Coronary heart disease is no longer just a disease of middle-aged and elderly people. appreviewpros.com will take you through an in-depth analysis of trends, symptom identification, risk management, interventional treatment, rehabilitation methods and personalized medication, and also correct some long-standing misconceptions in society.
The number of patients continues to rise, and the disease is increasingly affecting younger people.
If a decade or so ago, most coronary heart disease (CHD) patients were concentrated in the middle-aged and elderly, now, it’s no longer uncommon for young and middle-aged adults in their thirties and forties to be affected. The public perceives the onset of the disease in young people as sudden, largely because they don’t realize that CHD is not a “sudden illness,” but rather the result of the long-term accumulation of multiple risk factors. The overall incidence of CHD is rising, driven not only by population aging but also by the cumulative effects of long-term lifestyle changes and chronic disease management.
“Staying up late, prolonged sitting, eating takeout, smoking, high-fat diets, high emotional stress, and lack of physical examinations—these factors bring forward risks that would normally manifest in people in their fifties or sixties by ten or twenty years.” However, the middle-aged and elderly still constitute the majority of cases, although the age boundaries are no longer as clear as before.
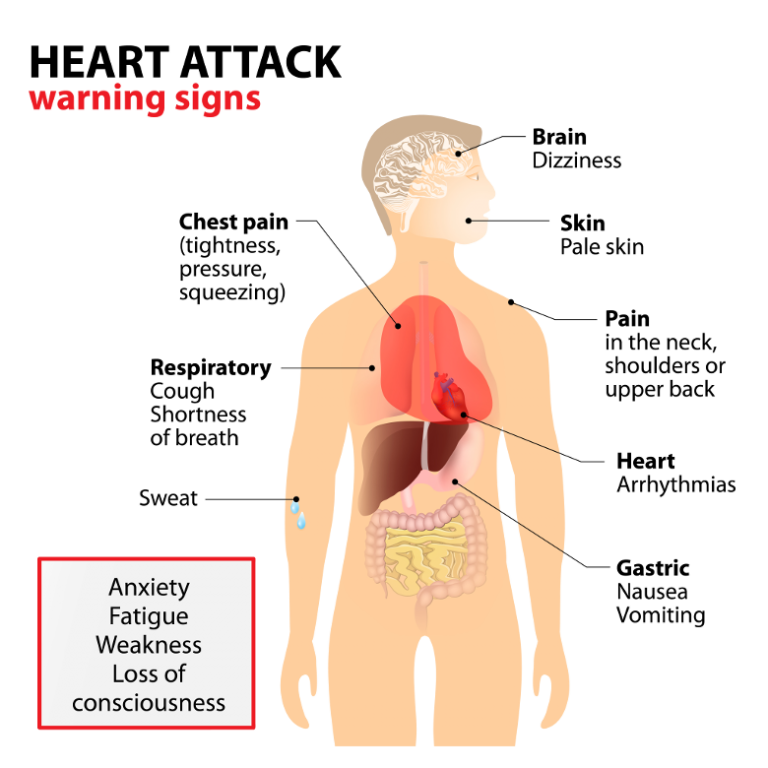
Chest pain ≠ myocardial infarction: Which signals require medical attention?
Chest pain is the symptom most commonly associated with CHD. While CHD and acute myocardial infarction can indeed cause chest pain or tightness, conversely, chest pain does not necessarily indicate cardiovascular problems. In large tertiary hospitals, less than one-third of patients diagnosed with CHD in the emergency room for chest pain are ultimately diagnosed with coronary heart disease. However, this doesn’t mean caution is unnecessary; rather, it requires a clearer identification of the characteristics of cardiogenic pain.
If a person can pinpoint a specific point of pain in their chest, the pain is often not from the heart, as the heart is an internal organ and its pain localization is not precise. Similarly, sharp, electric shock-like pain lasting only a second or two, or a fleeting throbbing sensation, is usually not indicative of ischemia and is more common in muscles, nerves, or superficial tissues. Chest pain truly caused by myocardial ischemia is most easily triggered by exercise, brisk walking, climbing stairs, or carrying heavy objects. It tends to last longer, gradually subsiding with rest, and in severe cases, may be accompanied by chest tightness, cold sweats, throat discomfort, or radiating pain to the shoulders, jaw, or teeth.
Patients don’t need to self-diagnose all types of pain, but if chest discomfort lasts longer than twenty minutes, is accompanied by difficulty breathing, nausea, throat tightness, or radiating pain, don’t hesitate to seek medical attention. “Especially for people with hypertension, diabetes, dyslipidemia, obesity, smoking habits, or a family history of cardiovascular disease, if they experience sudden chest pain but cannot pinpoint its location or nature, they should seek medical attention as soon as possible.”
Who are at high risk? Both controllable and uncontrollable factors need attention.
Regarding high-risk groups, risk factors for coronary heart disease (CHD) are divided into two categories: “unchangeable” and “changeable.” Age, gender, and family history are uncontrollable background variables. For example, the incidence rate is higher in men than in women during their youth and middle age, but gradually catches up in women ten years after menopause. The influence of genetic factors cannot be ignored; the cumulative effect of multiple genes is evident in some families. High blood pressure, high blood sugar, and high cholesterol, smoking, obesity, lack of exercise, emotional stress, and an unbalanced diet are all “accelerators” of CHD progression.
Many people still habitually treat chronic diseases as “short-term intervention diseases,” expecting to “take medication for several years at once” or “stop medication after two months of control.” This is a dangerous misconception. “Hypertension, hyperglycemia, and hyperlipidemia are not colds or pneumonia. They cannot be cured in essence, only controlled long-term. If well controlled, the risk is suppressed; if they fluctuate repeatedly, they are planting time bombs for CHD.”
The target for lipid control in CHD patients is not a one-size-fits-all approach, but rather tiered management. For example, for people without risk factors, LDL cholesterol should be kept below 3.4; if they have hypertension or carotid artery plaques detected by ultrasound, it needs to be lowered to below 2.6; once diagnosed with coronary heart disease or has undergone stent placement, the target value is below 1.8; if they have had a myocardial infarction, diabetes, multivessel disease, or even stroke, it should be lowered to below 1.4. “Some people think the numbers are unrealistically low, but the higher the risk, the less they can afford the continued attack of high cholesterol.”
How to Recover After Stent Placement? Don’t Treat Yourself Like a Sickly Person
When discussing coronary heart disease, stents are inevitably mentioned. One of the biggest misconceptions is that “if a blood vessel is blocked, you need a stent” or “after a stent is placed, you’re immune to heart attacks.” Stents only truly function in two situations: first, when an acute myocardial infarction occurs, requiring emergency opening of the blood vessel to prevent extensive myocardial necrosis; second, when significant exertional angina occurs, affecting daily life and cardiac function. “If a person’s blood vessel is 70-80% blocked but has no symptoms, and doesn’t experience recurring chest tightness or pain, then preventative stent placement won’t reduce their probability of a heart attack. A heart attack doesn’t essentially occur when the blockage reaches 80-90%, but rather when a plaque ruptures and forms a thrombus, blocking the blood vessel.”
Stents are not a “preventative measure” and will not replace medication. Many people worry that “stent placement means lifelong medication.” “Whether a heart attack patient has a stent or not, they still need to take medication. Lipid-lowering drugs, antiplatelet drugs, and blood pressure and blood sugar control are all essential.” If a patient has a stent placed without a heart attack but only due to stenosis symptoms, they may only add two antiplatelet drugs for a period after the procedure; the long-term treatment plan still reverts to managing the underlying disease. Regarding post-operative life, a concern for patients, those without myocardial infarction or heart failure recover well and can live and exercise like normal people. “Many people mistakenly believe that having a stent implanted means they can’t move; this is a misconception. What truly limits their activity isn’t the stent itself, but the chest pain they experienced before treatment.” Post-operatively, patients can gradually resume moderate-intensity exercises such as jogging, cycling, and swimming, while avoiding extreme stimulation such as saunas, bungee jumping, extreme roller coasters, and deep-sea diving. If heart failure is present, an exercise prescription needs to be developed under the guidance of a doctor and rehabilitation specialist to control heart rate and exercise load, gradually restoring function.