“My child always sleeps with their mouth open, is it because of enlarged adenoids?” “Their face shape has changed, is it adenoid facies?” In recent years, adenoid facies has frequently appeared on social media, attracting the attention of many parents. So, what is adenoid facies? Does it really affect a child’s development? How can parents detect it early and deal with it scientifically?
“Adenoid Facies”: More Than Just a Facial Issue
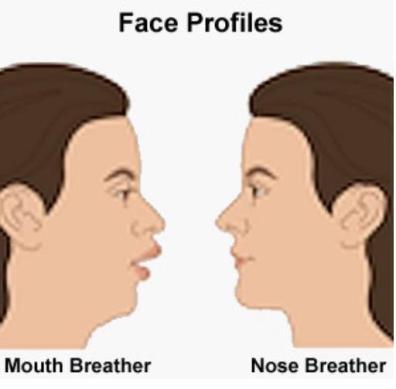
Adenoid facies is not an independent disease, but rather a dental and maxillofacial developmental abnormality caused by conditions such as enlarged adenoids and tonsils leading to upper airway obstruction and mouth breathing. Typical manifestations of this facial feature include upturned lips, thick lips, protruding incisors, receding mandible, malocclusion, and a high-arched hard palate. He pointed out that if a child already exhibits obvious adenoid facies, it indicates that the airway obstruction has persisted for a considerable period, and the skeletal structure has already changed. Intervention at this point is often less effective than earlier treatment.
The impact of sleep apnea goes far beyond facial changes. Persistent mouth breathing and intermittent hypoxia at night can interfere with the secretion of important hormones such as growth hormone, thus affecting a child’s height development, metabolic function, and potentially even causing damage to the cardiovascular system. Furthermore, disrupted sleep structure can also affect cognitive function. Clinically, some children with moderate to severe sleep apnea have lower scores on cognitive function and behavioral tests. Whether cognitive function can fully recover after treatment is currently inconclusive.
For parents, early detection of potential problems in their children is crucial.
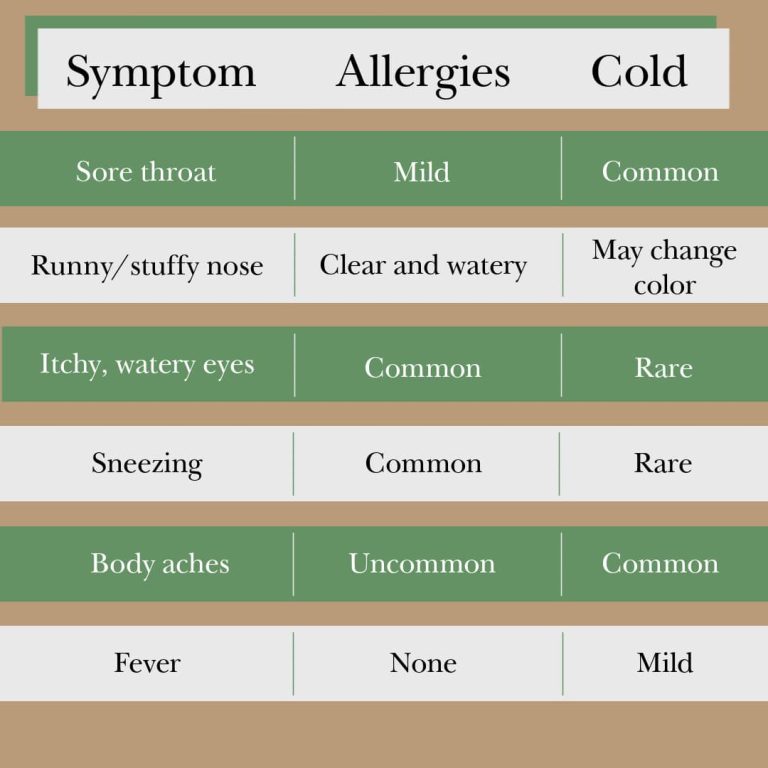
Persistent mouth breathing and snoring are two of the most easily observed characteristic signs. If a child habitually breathes through their mouth, or experiences persistent snoring or heavy breathing during sleep, it should be taken seriously. Occasional mouth breathing or snoring due to a cold is not a cause for excessive concern, but if these symptoms persist for several weeks or longer, a medical evaluation is necessary.
Clinically, adenoid hypertrophy and allergic rhinitis often coexist.
Approximately half of children who undergo adenoid surgery also have allergic rhinitis. Long-term nasal discharge regurgitation caused by allergic rhinitis can further worsen adenoid hypertrophy.
Many parents hesitate about whether to proceed with surgery for adenoid hypertrophy.
This requires considering multiple factors, including the child’s age, the degree of adenoid hypertrophy, the extent of facial changes, and the presence of sleep apnea. If facial changes are significant and airway obstruction is severe, surgery is more necessary. It’s important to note that if facial changes are limited to misaligned teeth, orthodontic treatment may be possible later. However, if the changes have affected the development of the entire nasomaxillofacial skeleton, orthodontic treatment alone may not achieve the desired results.
Multidisciplinary collaboration is needed to scientifically address adenoid facies.
Adenoid facies and sleep apnea involve multiple disciplines, and consulting a single department often fails to provide the most suitable solution.
Adenoid facies does not develop overnight, nor does it disappear on its own. Parents should pay attention to their child’s breathing patterns and sleep patterns, intervening promptly when the problem is still in its early stages and only manifests as soft tissue changes, rather than waiting until facial changes are obvious and irreversible changes in bone structure occur before seeking treatment. If a child has a long-term habit of mouth breathing or snoring, it is recommended to have a comprehensive evaluation at a multidisciplinary clinic as soon as possible for a scientific approach to safeguard the child’s healthy growth.