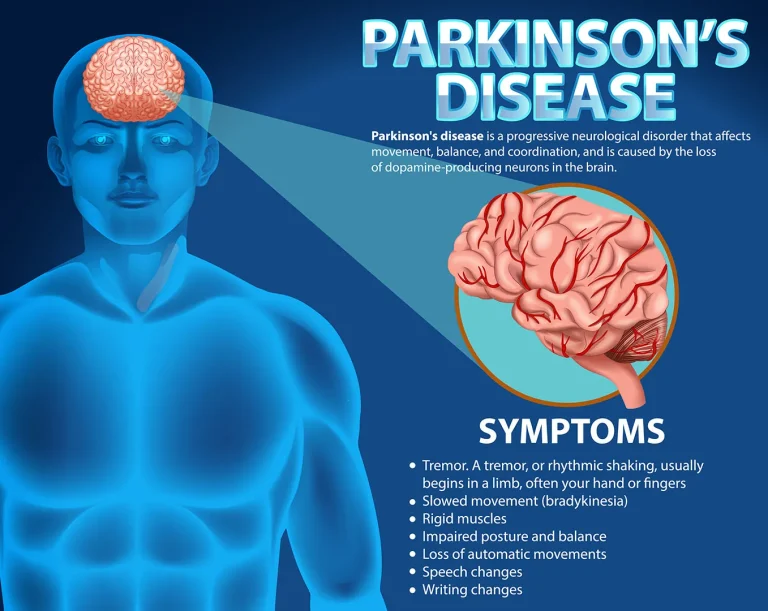
Parkinson’s disease (PD) is a common neurodegenerative disease affecting middle-aged and elderly people, typically beginning between the ages of 50 and 65. Its main symptoms include slowed movement, involuntary tremors of the hands, head, or mouth at rest, muscle rigidity, loss of flexibility and stiffness, and postural instability. Symptoms often begin on one side of the body and gradually spread to the other side or the whole body. In the late stages of the disease, patients become bedridden and unable to care for themselves. The core symptom of Parkinson’s disease is bradykinesia, such as slowed arm swings when walking, getting up, and turning over; difficulty with fine motor skills like brushing teeth; and abnormal gait, such as shuffling steps, lack of normal arm swing, and unsteady gait when turning. In addition, Parkinson’s disease has many non-motor symptoms, including decreased sense of smell, depressed mood, and sleep disturbances, with anxiety and depression being the most common. Approximately 70% of Parkinson’s patients experience anxiety symptoms, feeling tense and restless; about 50% have depressive symptoms, manifested as decreased interest, loss of appetite, and fatigue.
Parkinson’s disease (PD) is the third leading cause of death among middle-aged and elderly people after cancer and cardiovascular diseases, severely impacting patients’ work ability and quality of life. To date, the etiology of primary Parkinson’s disease remains incompletely understood. The main risk factors are aging, genetic factors (approximately 15% of patients have a family history), and oxidative stress, such as mental stress and arteriosclerosis. Currently, there is no cure for Parkinson’s disease; it is a chronic, progressive disease, and without timely treatment, patients’ lifespan is significantly shortened.
Early diagnosis of Parkinson’s disease is challenging. However, in recent years, the application of biomarker detection technologies (such as α-synuclein detection), high-resolution MRI imaging, novel PET tracers, and gut microbiota analysis has provided strong evidence for early diagnosis of PD, improving diagnostic accuracy.
Currently, Parkinson’s disease is treated with a multidisciplinary approach, including drug therapy, surgery, stem cell therapy, small molecule drug therapy, immunotherapy, non-drug interventions, gut probiotics/microbiota transplantation, rehabilitation therapy, and psychotherapy. Drug therapy is the first-line treatment. “Early diagnosis and early treatment” is the guiding principle for medication. Medication administration should adhere to “dosage titration” to avoid side effects and strive to achieve the goal of “achieving satisfactory clinical results with the lowest possible dose.” After 3-5 years of taking levodopa-like drugs, Parkinson’s disease patients may experience various motor complications such as on-off phenomena, end-of-dose phenomena, and dyskinesia. In these cases, a specialist should adjust the dosage and type of medication, or deep brain stimulation (DBS) may be used to improve these symptoms.
Currently, deep brain stimulation (DBS) is used clinically to treat Parkinson’s disease patients who are unresponsive to medication or have severe complications. DBS, commonly known as a brain pacemaker, is a landmark new technology in the surgical treatment of Parkinson’s disease. It involves implanting tiny electrodes in the brain to deliver electrical pulses to stimulate brain nuclei, thereby controlling the patient’s symptoms. Clinical studies have shown that most patients experience a significant reduction in medication dosage and a marked improvement in mobility after surgery. In 2025, a Stanford University research team published a clinical trial report on long-term personalized adaptive deep brain stimulation (aDBS) for Parkinson’s disease. The study confirmed that long-term aDBS application in a home environment demonstrates good tolerability, efficacy, and safety, allowing for real-time adjustment of stimulation intensity to achieve on-demand treatment and reduce over- or under-stimulation. The study showed that compared to traditional continuous deep brain stimulation (cDBS), aDBS maintained similar therapeutic efficacy, significantly reducing total energy output, improving battery life, and reporting reduced symptom fluctuations and improved motor symptoms. This research provides important clinical evidence for personalized, closed-loop neuromodulation therapy for Parkinson’s disease.
Novel treatment methods for Parkinson’s disease include: First, using artificial intelligence and the internet for comprehensive management of Parkinson’s patients, including telemedicine, wearable devices (bracelets) for monitoring and assessment, using smartphones to collect information and conduct public education, and using virtual reality technology for rehabilitation training; second, stem cell therapy: midbrain dopaminergic cells differentiated from human induced pluripotent stem cells (hiPSCs) have shown some efficacy in phase 1/2 trials; third, novel small molecule drugs for early intervention in Parkinson’s disease; fourth, immunotherapy: monoclonal antibody drugs, etc., for treating early-stage Parkinson’s patients; fifth, non-pharmacological interventions: transcranial magnetic stimulation (TMS) can improve motor and non-motor symptoms; magnetic resonance-guided focused ultrasound (MRgFUS) is used to treat tremor-type Parkinson’s disease; sixth, gut microbiota transplantation: regulating gut microbiota can reduce neuroinflammation and slow PD progression.
Rehabilitation therapy requires guidance from a rehabilitation therapist. Gentle exercises such as Tai Chi are suitable for Parkinson’s patients. Home care for Parkinson’s disease patients should include the following: prevent injuries; purchase a bedside toilet for easy access at night; use non-slip mats to secure dishes for safer eating; place non-slip mats on bathroom floors and in the bathtub; and ideally, sit while showering; choose clothing that is easy to put on and take off, with a front opening and zipper, and consider adding a small loop or string to the zipper for easier pulling; and choose shoes that do not require laces.
Four exercises to self-assess your Parkinson’s disease risk:
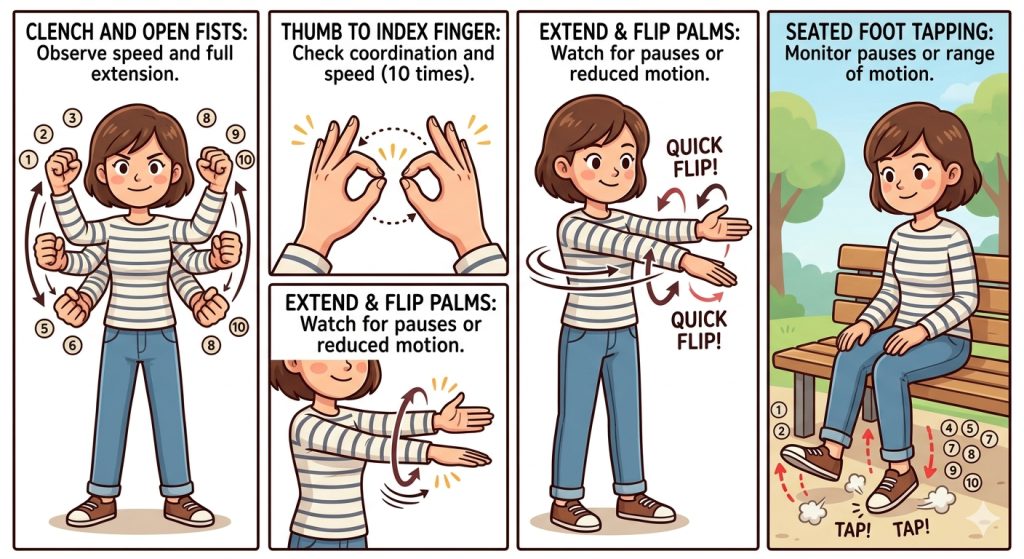
- Clench and open your fists as quickly as possible, doing this 10 times. Observe if you slow down or have any hands that cannot be fully opened.
- Touch your thumbs and index fingers together as quickly as possible, doing this 10 times. Observe if your hand movements are coordinated.
- Extend both arms and hands, and flip your palms and backs of your hands. Observe if there are any pauses or decreases in the range of motion.
- While seated, alternately raise one foot, repeatedly touching the ground with your toes. Do this 10 times. Observe if there are any pauses or a decreasing trend in the range of motion.