Spring breezes bring warmth, making it the perfect time for outings, but persistent sneezing, itchy nose, itchy eyes, and other allergy symptoms dampen the spirits of many.
How to distinguish between allergies and a cold? How to deal with rhinitis, itchy eyes, and skin allergies?
Allergies or a cold: how to quickly tell the difference?
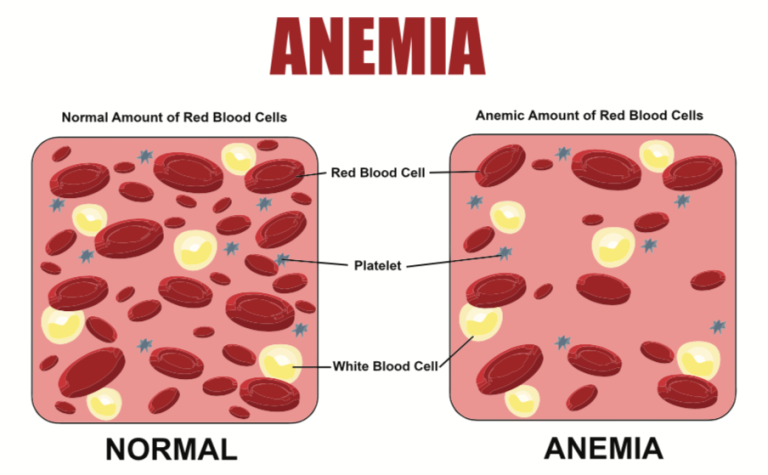
Many people experience sneezing, runny nose, and itchy eyes in spring, but can’t tell if it’s an allergy or a cold.
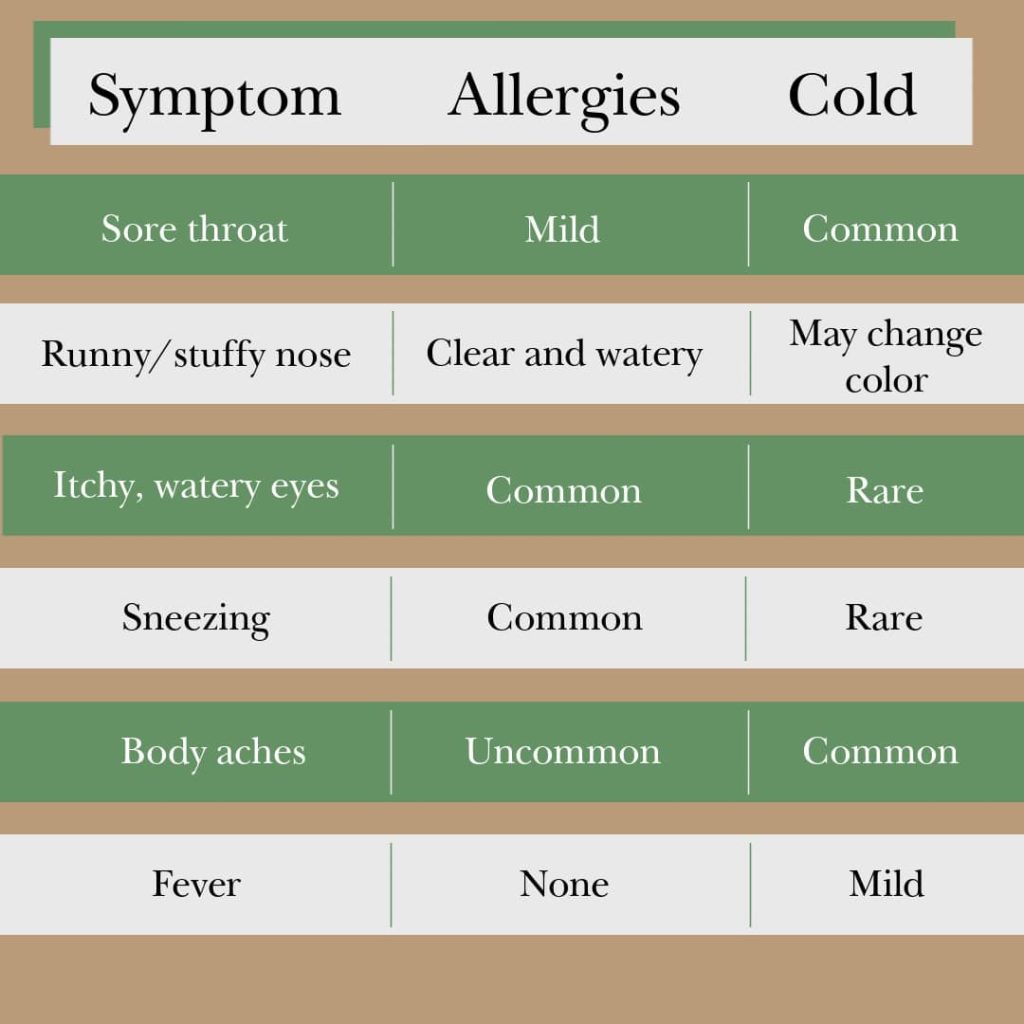
While colds and allergies do share similarities, such as sneezing and runny nose, there are still significant differences: colds are often accompanied by systemic symptoms like fever, sore throat, and muscle aches, but generally don’t cause itching; allergies, on the other hand, primarily manifest as significant itching in the eyes and nose, and often occur at a fixed time each spring or autumn.
In terms of course, colds are self-limiting illnesses, usually resolving on their own within about a week; allergies, however, are closely related to allergen exposure. Those with pollen allergies experience symptoms during specific seasons, while those with dust mite allergies may experience recurring symptoms throughout the year.
How to protect yourself from spring allergies?
People with a known history of pollen allergies should pay attention to pollen concentration forecasts and reduce outdoor activities when concentrations are high. When going out, wear masks, goggles, and long-sleeved clothing. Use pollen blockers in your nasal passages or take preventative medication under the guidance of a doctor. Shake off any dust before going home, change your outer clothing promptly upon arrival, and clean your face and nasal passages. Close doors and windows, turn on air purifiers to reduce indoor pollen levels, and apply cold compresses if necessary to alleviate symptoms and help you get through the allergy season smoothly.
Mild Symptoms? Ignore Them! Early Intervention is Key
Many patients with mild pollen allergy symptoms face a dilemma: should they “tough it out” during pollen season, or seek treatment as soon as possible?
Mild symptoms present the best opportunity for early intervention. Past experience shows that without control, most patients’ symptoms gradually worsen. Therefore, timely and standardized drug treatment at the onset of symptoms is crucial to preventing a decline in quality of life and helping patients return to a normal life.
Allergy treatment should follow a standardized and regulated approach. For allergic rhinitis, the preferred treatment is nasal corticosteroids combined with antihistamines. Many patients still have concerns about corticosteroids. It’s important to understand that nasal corticosteroids are topical medications that act directly on the nasal mucosa, quickly relieving symptoms such as runny nose, sneezing, nasal congestion, and nasal itching. Systemic absorption after nasal administration is very low, making it very safe with proper use and unlikely to cause long-term dependence. Patients are advised to consistently use medication throughout the pollen season.
In terms of treatment strategies, allergic rhinitis follows a stepwise approach: for mild cases, topical medications are the first-line treatment, with nasal corticosteroids as the primary option; if topical medications are ineffective, systemic medications can be considered, such as oral antihistamines or leukotriene receptor antagonists, forming a standardized combination of topical and systemic medications. If symptoms persist for more than a week after the above-mentioned standardized treatment and reach the criteria for moderate to severe symptoms, i.e., significantly affecting work, study, daily life, or sleep, further escalation of treatment is indicated.
Don’t Ignore Itchy Eyes; Damaging Your Cornea Can Be Regrettable
During allergy season, some patients experience symptoms such as red, itchy, and watery eyes. This not only affects visual quality but, if left uncontrolled, can also damage the structure and function of the cornea. Studies suggest that recurrent and persistent allergies are a significant risk factor for keratoconus, making standardized treatment crucial.
Treatment of eye allergies also employs a step-by-step strategy. The first step is to avoid contact with allergens. This can be achieved through human intervention to reduce exposure or by actively avoiding allergenic environments, such as temporarily migrating from the north to the south during pollen season.
The second step is to use medication as prescribed by a doctor. Treatment primarily involves ophthalmic anti-allergy medications, including antihistamines and dual-action drugs. Dual-action drugs stabilize immune-related cells, reducing the release of inflammatory mediators, while simultaneously antagonizing already released mediators, thereby alleviating symptoms such as red, itchy, and watery eyes caused by allergies. For more severe cases involving T lymphocytes, upgraded treatment plans are necessary. Some critically ill patients may use steroid eye drops for a short period of time, but it is generally recommended to limit use to 2 to 4 weeks, and have their intraocular pressure monitored regularly by a doctor during the medication period.
Common Misconceptions About Allergy Medication
Regarding common misconceptions in allergy management, several experts offer the following three tips:
First, Self-medicating with “popular online eye drops.” Many patients buy vasoconstrictor eye drops on their own. While these medications can relieve symptoms in the short term, they don’t address the root cause of the allergy. After the effects wear off, reflexive vasodilation can release more inflammatory mediators, worsening damage to the ocular surface.
Second, Misusing steroid eye drops. Some patients know that steroids are necessary for allergies and buy and use them on their own. However, steroid medications are a double-edged sword: nasal steroids are relatively safe and can be used long-term; while ocular steroids carry higher risks and must be used short-term under a doctor’s guidance, with regular monitoring of intraocular pressure. Otherwise, they may cause irreversible visual damage such as steroid-induced glaucoma.
Third, Believing that warm compresses can relieve eye discomfort caused by allergies. Different eye diseases require different nursing methods. For example, while warm compresses are often used to promote glandular secretion in dry eyes, they can actually worsen symptoms in allergies by increasing blood circulation in the eyes, especially during acute episodes. The correct approach is to first apply a cold compress to relieve discomfort by constricting blood vessels.